
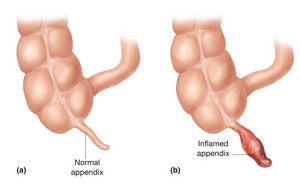
The appendix (see picture below) is a largely useless part of the bowel in the human, measuring around 10cm in length in an adult. However, some species of animal cannot be without it - for example the rabbit - as the grass that a rabbit eats needs time to be broken down further to extract the maximum benefit from digesting cellulose. Hence the diameter and length is 3-5 times that of the human, as it is common in herbivores.
How common appendicitis it is in rabbits is unclear(!) but it is a significant cause of illness in humans, with over 35,000 patients in the UK being treated for this condition on a yearly basis.
In the USA, 250,000 patients have their appendixes removed, so it is an important problem with its own complications should delay, mis-diagnosis or a failure to diagnose it at all, occur. The small bowel joins the large bowel at the ileo-caecal junction; the small bowel is involved with enzymatic breakdown of food whilst the main role of the large bowel is to absorb water and make stool.
Just beyond the junction, the appendix dangles down (but sometimes, it does not dangle but goes up behind the ascending colon which can complicate the clinical picture). The appendix is a blind ended part of the bowel that has its own blood supply, the appendicular artery and vein as well as associated lymph glands.
The appendix becomes inflamed in appendicitis – this may be due to blockage of the outlet of the appendix and inflammation develops in the surrounding tissues. The lymph glands enlarge and the blood flow to the appendix increases at first. The wall of the appendix becomes engorged and may become thinned and can then rupture.
The classic signs of appendicitis are a low temperature with abdominal pain, that starts near the belly button and then it goes down to the right lower part of the abdomen, called the right iliac fossa, at McBurney’s point.
The lining of the abdomen and its organs are covered by a thin membrane, the peritoneum which contains pain fibres. When the peritoneum becomes irritated (this may be due to the inflamed appendix coming into contact with the peritoneum), then there is localised tenderness in this area. If the appendix bursts, pus may disperse throughout the abdomen causing peritonitis, inflammation of the lining of the abdomen, which means that it is difficult to move the abdomen as it hurts a lot!
In children it can be difficult to diagnose – for example when the child is not able to communicate or when the appendix is not located in the usual position but rests up against the back wall of the abdomen (the retro-caecal appendix) when there may be back pain.
Another variation is that the appendix bursts but becomes enclosed in the ‘fatty apron’, known as the omentum. This can seal off the appendix, enveloping it so that pus does not disperse but is contained. This is known as an appendicular abscess. This requires intravenous antibiotics and eventual removal. In the USA, it is estimated that between 30-50% of cases are mis-diagnosed so it is not surprising that it is the 5th most common cause of medico-legal litigation in the USA.
Treatment of acute appendicitis is surgical after the diagnosis is suspected. This will be by clinical judgement; sometimes investigations such as ultrasound to look at the appendix and the blood flow to it with confirmation of a raised white cell count may assist with the diagnosis. The ultimate diagnosis is made by histological confirmation showing the presence of infection in the tissues of the appendix.
It has a high morbidity in the very young, e.g. in the neonatal period. Delay in making the diagnosis can lead to peritonitis and eventually death as peritonitis can lead to invasion of bacteria and inflammatory products into the circulation.
Medico-legal Considerations
Acute appendicitis has to be considered a cause of abdominal pain in young people. The features may not be those as classically described but if it is not considered then the risk of morbidity and mortality increases significantly.
Modern surgical advances mean that laparascopic techniques are employed in most cases, decreasing the risk of wound breakdown and lessening intra-abdominal infection. In complicated cases, there may have to be an opening of the abdominal wall, a laparotomy, to get to the appendix and deal with the infection associated with the infection.
For a child or young person who present to the emergency department with abdominal pain, the examination should include looking for the symptoms and signs of acute appendicitis which include tenderness, initially localised to be around the umbilicus and then moving down to the right side of the lower abdomen. There may be a low grade fever, an increased heart rate and if, blood tests are performed, there may be a raised white cell count. Surgical opinion should be sought, and other investigations such as an ultrasound may be requested.
It is common practice in the US for an abdominal CT scan to be performed but the risk/benefit consideration in the UK means that this is not part of the routine investigations for this condition.
If you want further information about this particular topic, or wish to discuss the possibility of bringing a claim for Clinical Negligence - or indeed any other type of injury, please contact the Dutton Gregory Clinical Negligence Team on (01202) 315005, or email k.marden@duttongregory.co.uk
NB This article does not constitute legal advice and should not be relied on as such. No responsibility for the accuracy and/or correctness of the information and commentary set out in the article, or for any consequences of relying on it, is assumed or accepted by any member of Dutton Gregory, Solicitors.




